

Clinical Study of Acupuncture Therapy as An Auxiliary Treatment for Guillain-Barre Syndrome
-
摘要:
目的 观察针刺疗法辅助治疗格林巴利综合征(GBS)的临床疗效。 方法 以三亚市中医院2019年2月—2021年10月收治的169例GBS患者为研究对象, 随机数字表法分为对照组(83例)和观察组(86例), 其中西药对照组50例, 西药观察组50例, 中药对照组33例, 中药观察组36例。对照组给予常规西药或中药治疗, 观察组在对照组治疗基础上另给予针刺辅助治疗, 疗程4周。比较治疗前后对照组和观察组四肢肌力、神经功能[运动神经传导速度(MCV)、感觉神经传导速度(SCV)]、中医证候积分、临床疗效、血清炎性因子[白介素-10(IL-10)、白介素-18(IL-18)]水平及安全性指标变化情况。 结果 治疗后, 西药、中药观察组四肢肌力明显升高(P < 0.05, P < 0.01), 优于对照组(P < 0.05);西药、中药观察组正中神经、胫神经MCV、SCV明显升高(P < 0.05), 优于对照组(P < 0.05);西药、中药观察组中医证候评分明显低于治疗前, 并低于对照组(P < 0.05);西药、中药观察组治疗总体有效率明显高于对照组(P < 0.05);西药、中药观察组IL-10水平明显升高(P < 0.01), 并高于对照组(P < 0.05), IL-18明显降低(P < 0.01), 并低于对照组(P < 0.05);各组均无明显并发症。 结论 针刺辅助疗法能够明显提高西药、中药治疗的临床疗效, 改善患者肌力、神经功能及临床症状, 恢复患者血清炎症因子水平。 Abstract:OBJECTIVE To observe the clinical efficacy of acupuncture therapy in the auxiliary treatment of Guillain-Barre syndrome (GBS). METHODS A total of 169 patients with GBS admitted to Sanya TCM Hospital from February 2019 to October 2021 were studied, and were divided into control group (83 cases) and observation group (86 cases) by random number table method. There were 50 cases in the western medicine control group, 50 cases in the western medicine observation group, 33 cases in the Chinese medicine control group, and 36 cases in the Chinese medicine observation group. The control group was treated with conventional western or Chinese medicine therapies, while the observation group was given acupuncture-auxiliary treatment based on the therapies in the control group. The treatment course lasted four weeks. In addition, we compared the muscle strength of the limbs, nerve function [motor nerve conduction velocity (MCV), sensory nerve conduction velocity (SCV)], traditional Chinese medicine (TCM) syndrome scores, clinical efficacy, serum inflammatory factors [interleukin-10 (IL-10), interleukin-18 (IL-18)] levels, as well as safety indexes in the control group and the observation group before and after treatment. RESULTS After treatment, the muscle strength of the of limbs was significantly increased in the western and Chinese medicine observation groups (P < 0.05, P < 0.01), whose results were better than those in the control group (P < 0.05). Besides, the MCV and SCV of the median nerve and tibial nerve were significantly increased in the western and Chinese medicine observation groups (P < 0.05), whose results were also better than those in the control group (P < 0.05). In addition, TCM syndrome scores were significantly reduced in the western and Chinese medicine observation groups compared to pre-treatment results and lower than those in the control group (P < 0.05). The total effective rates of treatment in the western and Chinese medicine observation groups were significantly increased than those in the control group (P < 0.05). on top of that, the IL-10 levels in the western and Chinese medicine observation groups were significantly increased (P < 0.01) and higher than those in the control group (P < 0.05), while IL-18 levels were significantly reduced (P < 0.01) and lower than those in the control group (P < 0.05). There were no notable complications in all groups. CONCLUSION Acupuncture auxiliary therapy can significantly optimize the clinical efficacy of western and Chinese medicine treatment. Besides, it can improve patients' muscle strength and neurological function, mitigate clinical syndromes, and restore patients' serum inflammatory factor levels. -
Key words:
- Guillain-Barre syndrome /
- acupuncture /
- auxiliary treatment
-

图 1 4组患者治疗前后四肢肌力得分比较
注: 组内比较, *P < 0.05, **P < 0.01;组间比较, ΔP < 0.05。x±s,n西药对照组=50, n西药观察组=50, n中药对照组=33, n中药观察组=36。
Figure 1. Comparison of muscle strength scores of the four groups of patients before and after treatment

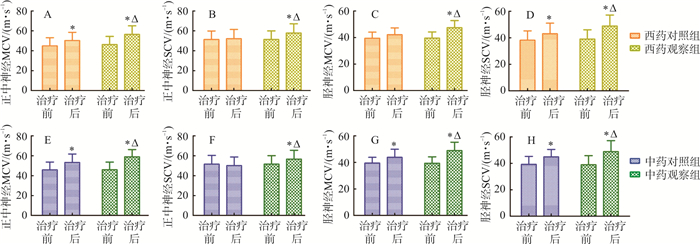
图 2 4组患者治疗前后神经功能比较
注: 组内比较, *P < 0.05;组间比较, ΔP < 0.05。x±s,n西药对照组=50, n西药观察组=50, n中药对照组=33, n中药观察组=36。
Figure 2. Comparison of neurological function of the four groups before and after treatment

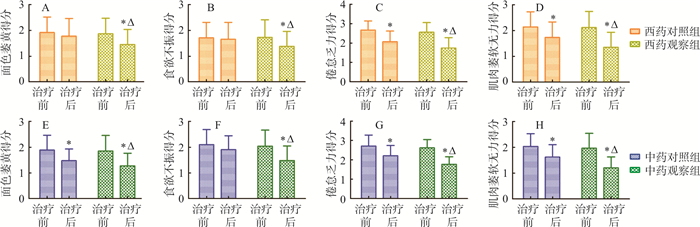
图 3 4组患者治疗前后中医证候积分比较
注: 组内比较, *P < 0.05;组间比较, ΔP < 0.05。x±s,n西药对照组=50, n西药观察组=50, n中药对照组=33, n中药观察组=36。
Figure 3. Comparison of TCM syndrome scores of the four groups before and after treatment
表 1 4组患者基线资料比较(x±s)
Table 1. Comparison of baseline information of patients in the four groups (x±s)
组别 例数 性别 年龄/岁 病程/月 休斯功能分级量表 男 女 1级 2级 3级 4级 西药对照组 50 29 21 28.53±5.49 9.16±2.63 6 17 20 7 西药观察组 50 30 20 28.23±5.54 9.28±2.69 6 16 21 7 中药对照组 33 18 15 31.46±6.21 8.48±2.41 5 11 13 4 中药观察组 36 20 16 30.23±4.93 8.75±1.43 4 14 15 3 注: 病情严重程度采用休斯功能分级量表(Hughes functional grading scale, HFGS)[11]评分: 6分为死亡; 5分为需要呼吸机辅助呼吸; 4分为卧床; 3分为步行5 m需要帮助; 2分为可自行行走; 1分为轻微症状或体征; 0分为正常。4级: 评分≤1分, 3级: 2~3分, 2级: 3~4分, 1级: >4分。  下载: 导出CSV
下载: 导出CSV
表 2 4组患者治疗后中医临床疗效比较
Table 2. Comparison of clinical efficacy of TCM after treatment in the four groups
组别 例数 治愈 好转 未愈 有效率/% 西药观察组 50 28 21 1 98.00* 西药对照组 50 20 19 11 78.00 中药对照组 33 11 15 7 78.79 中药观察组 36 14 19 3 91.67* 注: 组间比较, χ西药组2=5.28, χ中药组2=5.13, *P < 0.05。
下载: 导出CSV
表 3 4组患者治疗前后血清炎性因子水平比较(x±s, pg·mL-1)
Table 3. Comparison of serum inflammatory factors before and after treatment in the four groups (x±s, pg·mL-1)
组别 例数 时间 IL-10 IL-18 西药对照组 50 治疗前 46.23±5.94 135.43±28.47 治疗后 67.42±5.51** 66.47±15.33** 西药观察组 50 治疗前 46.15±5.84 135.52±28.54 治疗后 69.28±6.04**Δ 62.24±17.62**Δ 中药对照组 33 治疗前 45.28±6.31 134.86±26.97 治疗后 68.53±4.84** 63.87±6.74** 中药观察组 36 治疗前 45.83±5.59 135.93±27.35 治疗后 70.06±5.62**Δ 60.64±9.32**Δ 注: 组内比较, **P < 0.01;组间比较, ΔP < 0.05。
下载: 导出CSV
表 4 4组患者治疗前后安全性比较(x±s)
Table 4. Comparison of safety indexes before and after treatment in the four groups (x±s)
组别 例数 时间 WBC/(109·L-1) AST/(U·L-1) ALT/(U·L-1) GGT/(U·L-1) CR/(μmol·L-1) BUN/(μmol·L-1) UA/(μmol·L-1) 西药对照组 50 治疗前 5.96±1.69 25.12±2.91 27.65±3.23 14.13±4.36 81.12±11.78 4.53±0.70 230.19±31.59 治疗后 5.95±1.70 25.71±3.23 28.35±3.48 13.43±4.87 84.32±12.28 3.31±0.63 254.59±30.69 西药观察组 50 治疗前治疗后 6.02±1.61 24.78±2.87 24.56±3.15 13.93±4.96 70.04±14.91 3.91±0.76 274.61±38.72 治疗后 6.13±1.65 23.56±2.48 26.75±3.82 15.34±5.28 66.64±15.12 4.82±0.55 273.71±41.81 中药对照组 33 治疗前 6.05±1.67 25.98±3.13 27.62±4.21 13.85±4.12 78.21±13.22 4.31±0.59 246.39±32.78 治疗后 6.07±1.71 26.85±3.23 26.91±4.13 14.58±4.43 72.65±11.84 4.28±0.42 228.82±37.58 中药观察组 36 治疗前 5.98±1.69 25.51±3.02 26.05±3.78 13.55±4.17 67.81±15.82 5.71±0.47 258.57±31.63 治疗后 6.08±1.72 25.39±2.94 24.84±4.27 13.42±4.23 69.74±16.81 6.20±0.23 283.72±32.72
下载: 导出CSV
-
[1] FAN Z, LIU BY, ZHANG YL, et al. The effectiveness and safety of acupuncture therapy for Guillain-Barre syndrome[J]. Medicine, 2020, 99(2): e18619. doi: 10.1097/MD.0000000000018619 [2] 金泽, 徐婵娟, 刘甜甜, 等. 夹脊穴穴位埋线联合电针治疗格林巴利综合征24例临床研究[J]. 江苏中医药, 2019, 51(12): 70-72. doi: 10.3969/j.issn.1672-397X.2019.12.025JIN Z, XU CJ, LIU TT, et al. Clinical study on 24 cases of Guillain-Barre syndrome treated by catgut embedding at Jiaji acupoint combined with electroacupuncture[J]. Jiangsu J Tradit Chin Med, 2019, 51(12): 70-72. doi: 10.3969/j.issn.1672-397X.2019.12.025 [3] 郭芳, 张拥波, 王瑞金. 格林-巴利综合征/急性脊髓炎重叠综合征的临床特点及机制分析[J]. 临床和实验医学杂志, 2016, 15(4): 339-342. doi: 10.3969/j.issn.1671-4695.2016.04.013GUO F, ZHANG YB, WANG RJ. Clinical characteristics and mechanism analysis of GBS/AM overlap syndrome[J]. J Clin Exp Med, 2016, 15(4): 339-342. doi: 10.3969/j.issn.1671-4695.2016.04.013 [4] 郑爱华, 李飞燕, 黄义平, 等. 电针加中药内服结合康复训练治疗格林巴利综合征疗效观察及对功能恢复的影响[J]. 四川中医, 2017, 35(3): 174-176. https://www.cnki.com.cn/Article/CJFDTOTAL-SCZY201703068.htmZHENG AH, LI FY, HUANG YP, et al. Effect of electroacupuncture plus oral administration of traditional Chinese medicine combined with rehabilitation training on Guillain-Barré syndrome and its influence on functional recovery[J]. J Sichuan Tradit Chin Med, 2017, 35(3): 174-176. https://www.cnki.com.cn/Article/CJFDTOTAL-SCZY201703068.htm [5] MERKIES ISJ, KIESEIER BC. Fatigue, pain, anxiety and depression in guillain-Barré syndrome and chronic inflammatory demyelinating polyradiculoneuropathy[J]. Eur Neurol, 2016, 75(3/4): 199-206. [6] ALROHIMI A, JASSAL R. Headache in guillain-Barré syndrome: Diagnostic and management implications[J]. Can J Neurol Sci, 2018, 45(2): 240-242. doi: 10.1017/cjn.2017.247 [7] YANG L, ZHAO XM. Integrated Chinese and western medicine for acute Guillain-Barré syndrome treatment[J]. Transl Neurosci, 2020, 11: 38-47. doi: 10.1515/tnsci-2020-0007 [8] 熊兴江. 《千金要方》小续命汤治疗面神经炎、四肢无力、颈椎病、急性脊髓炎、急性神经根炎、格林巴利综合征、多发性硬化、重症肌无力、运动神经元病、皮肌炎体会[J]. 中国中药杂志, 2020, 45(12): 2735-2751. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZY202012002.htmXIONG XJ. Experience of treating facial neuritis, unexplained limb weakness, cervical spondylosis, acute myelitis, acute radiculitis, Guillain Barre syndrome, multiple sclerosis, myasthenia gravis, motor neuron disease, dermatomyositis with Xiaoxuming Decoction[J]. China J Chin Mater Med, 2020, 45(12): 2735-2751. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZY202012002.htm [9] 王征, 张虎, 张大尉. 针刺联合益气化瘀经验方对缺血性中风患者的肢体活动能力和认知能力的改善作用[J]. 四川中医, 2018, 36(10): 194-197. https://www.cnki.com.cn/Article/CJFDTOTAL-SCZY201810067.htmWANG Z, ZHANG H, ZHANG DW. Effect of acupuncture combined with Yiqi Huayu Decoction on improving limb activity and cognitive ability in patients with cerebral apoplexy[J]. J Sichuan Tradit Chin Med, 2018, 36(10): 194-197. https://www.cnki.com.cn/Article/CJFDTOTAL-SCZY201810067.htm [10] FOKKINK WJR, WALGAARD C, KUITWAARD K, et al. Association of albumin levels with outcome in intravenous immunoglobulin-treated guillain-Barré syndrome[J]. JAMA Neurol, 2017, 74(2): 189-196. doi: 10.1001/jamaneurol.2016.4480 [11] 白霞, 郑毅, 许鑫, 等. 激荡气血法配合丙种球蛋白治疗慢性格林巴利综合征疗效及对血清炎症因子的影响[J]. 现代中西医结合杂志, 2018, 27(12): 1322-1324. doi: 10.3969/j.issn.1008-8849.2018.12.019BAI X, ZHENG Y, XU X, et al. Effect of qi-blood stirring therapy combined with gamma globulin on chronic Guillain-Barré syndrome and its influence on serum inflammatory factors[J]. Mod J Integr Tradit Chin West Med, 2018, 27(12): 1322-1324. doi: 10.3969/j.issn.1008-8849.2018.12.019 [12] 中华医学会神经病学分会, 中华医学会神经病学分会周围神经病协作组, 中华医学会神经病学分会肌电图与临床神经电生理学组, 等. 中国吉兰-巴雷综合征诊治指南2019[J]. 中华神经科杂志, 2019, 52(11): 877-882. doi: 10.3760/cma.j.issn.1006-7876.2019.11.002Chinese Society of Neurology, Peripheral Neuropathy Collaboration Group of Chinese Society of Neurology, Chinese Society of Electromyography and Clinical Neuroelectrophysiology, et al. 2019 Chinese guidelines for diagnosis and treatment of Guillain-Barre syndrome[J]. Chin J Neurol, 2019, 52(11): 877-882. doi: 10.3760/cma.j.issn.1006-7876.2019.11.002 [13] 国家中医药管理局. 中医病证诊断疗效标准[M]. 南京: 南京大学出版社, 1994: 23-24.National Administration of Traditional Chinese Medicine. Therapeutic Standard of TCM Diagnosis of Diseases and Syndromes[M]. Nanjing: Nanjing university press, 1994: 23-24. [14] 毛俊雄. 实用神经内科诊疗学[M]. 石家庄: 河北科学技术出版社, 1999: 24.MAO JX. Practical Neurology Diagnosis and Treatment[M]. Shijiazhuang: Hebei science and technology press, 1999: 24. [15] 卢祖能. 实用肌电图学[M]. 北京: 人民卫生出版社, 2000: 273-339, 370-372.LU ZN. Practical Electromyography[M]. Beijing: People's medical publishing house, 2000: 273-339, 370-372. [16] 周霞, 孙中武. 吉兰-巴雷综合征的发病机制及诊治进展[J]. 中华全科医学, 2019, 17(4): 526-527. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY201904002.htmZHOU X, SUN ZW. Pathogenesis, diagnosis and treatment progress of Guillain-Barre syndrome[J]. Chin J Gen Pract, 2019, 17(4): 526-527. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY201904002.htm [17] CEA G, JARA P, QUEVEDO F. Clinical features of Guillain-Barré syndrome in 41 patients admitted to a public hospital[J]. Rev Med Chil, 2015, 143(2): 183-189. doi: 10.4067/S0034-98872015000200005 [18] 赵秀敏, 高长玉. 扶正清热复方联合常规疗法治疗急性吉兰-巴雷综合征疗效观察[J]. 中国中西医结合杂志, 2019, 39(12): 1440-1444. doi: 10.7661/j.cjim.20190425.008ZHAO XM, GAO CY. Effects of fuzheng Qingre formula combined with routine therapy on acute Guillain-Barré syndrome[J]. Chin J Integr Tradit West Med, 2019, 39(12): 1440-1444. doi: 10.7661/j.cjim.20190425.008 [19] 马伯俊, 吴志君, 林映欣. 强直性脊柱炎患者采用中药汤剂联合针灸治疗临床疗效研究[J]. 河北中医药学报, 2017, 32(5): 20-22. https://www.cnki.com.cn/Article/CJFDTOTAL-HZYX201705007.htmMA BJ, WU ZJ, LIN YX. Clinical efficacy of traditional Chinese medicine decoction combined with acupuncture in treating ankylosing spondylitis[J]. J Hebei Tradit Chin Med Pharmacol, 2017, 32(5): 20-22. https://www.cnki.com.cn/Article/CJFDTOTAL-HZYX201705007.htm [20] ALAM TA, CHAUDHRY V, CORNBLATH DR. Electrophysiological studies in the Guillain-Barre syndrome: Distinguishing subtypes by published criteria[J]. Muscle Nerve, 1998, 21(10): 1275-1279. doi: 10.1002/(SICI)1097-4598(199810)21:10<1275::AID-MUS5>3.0.CO;2-8 [21] 黄帝内经素问[M]. 北京: 人民卫生出版社, 2005: 88.The Yellow Emperor's Inner Classic: Basic Questions[M]. Beijing: People's medical publishing house, 2005: 88-89. [22] 汤晓芙. 临床肌电图学[M]. 北京: 人民卫生出版社, 1995: 56.TANG XF. Clinical Electromyography[M]. Beijing: People's medical publishing house, 1995: 56. [23] 陈冲. 针刺组穴对脑卒中后偏瘫病人神经功能及患肢肢体功能恢复的影响[J]. 内蒙古医科大学学报, 2019, 41(1): 78-80, 85. https://www.cnki.com.cn/Article/CJFDTOTAL-NMYX201901019.htmCHEN C. Effect of acupuncture on neurological function and limb function recovery of hemiplegic patients after stroke[J]. J Inn Mong Med Univ, 2019, 41(1): 78-80, 85. https://www.cnki.com.cn/Article/CJFDTOTAL-NMYX201901019.htm [24] 刘洪波, 方树友, 王玉萍, 等. 格林-巴利综合征患者脑脊液IL-10、IL-12水平的研究[J]. 中国免疫学杂志, 2007, 23(8): 725-726, 731. https://www.cnki.com.cn/Article/CJFDTOTAL-ZMXZ200708011.htmLIU HB, FANG SY, WANG YP, et al. Study on the levels of IL-10 and IL-12 in cerebrospinal fluid of patients with Guillain-Barré syndrome[J]. Chin J Immunol, 2007, 23(8): 725-726, 731. https://www.cnki.com.cn/Article/CJFDTOTAL-ZMXZ200708011.htm [25] 李清华, 王莉, 王克玲, 等. 白细胞介素18在格林巴利综合征病程中的变化[J]. 临床荟萃, 2007, 22(2): 92. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFC200702009.htmLI QH, WANG L, WANG KL, et al. Changes of interleukin-18 in the course of Guillain-Barre syndrome[J]. Clin Focus, 2007, 22(2): 92. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFC200702009.htm -

 点击查看大图
点击查看大图

计量
- 文章访问数: 114
- HTML全文浏览量: 15
- PDF下载量: 12
- 被引次数: 0
