

Clinical Efficacy and Mechanism of Lichang Beverage in the Treatment of Diarrhea-Type Irritable Bowel Syndrome with Liver Depression and Spleen Deficiency
-
摘要:
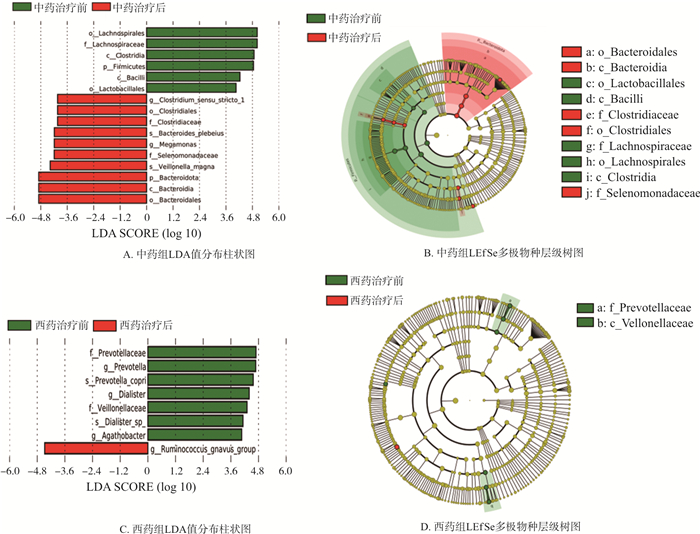
目的 基于菌-脑-肠轴观察理肠饮治疗腹泻型肠易激综合征(IBS-D)肝郁脾虚证的临床疗效及对血清脑肠肽、肠道菌群的影响, 探讨其可能的疗效机制。 方法 纳入66例IBS-D肝郁脾虚证患者, 以2 ∶ 1比例随机分为中药组44例和西药组22例, 中药组予理肠饮口服, 西药组予培菲康联合得舒特口服, 疗程均为4周, 评估治疗前、治疗2周、治疗4周2组患者的IBS症状严重程度量表(IBS-SSS)评分变化, 治疗前后观察2组患者中医症状积分变化情况, 检测血清脑肠肽指标[血清P物质(Substance P, SP)及5-羟色胺(Serotonin, 5-HT)]表达水平及肠道菌群的组成情况。 结果 ① 治疗2周、治疗4周, 2组IBS-SSS评分均显著降低(P < 0.01), 中药组优于西药组(P < 0.01);治疗4周后, 2组患者中医证候总积分均显著降低(P < 0.01), 中药组优于西药组(P < 0.01), 且中药组临床愈显率及总有效率均高于西药组(P < 0.05, P < 0.01)。②治疗后, 2组患者血清SP含量均明显下降(P < 0.05), 中药组血清5-HT含量显著下降(P < 0.01),2组比较无显著性差异(P>0.05)。③α多样性分析提示, 治疗后2组肠道菌群的丰富度不同程度下降(P < 0.05, P < 0.01), 西药组菌群多样性较前下降(P < 0.05), 而中药组较前无明显差异(P>0.05);PCoA分析提示2组微生物群落构成均发生明显改变(P < 0.05), 且组间比较具有显著差异(P < 0.01)。其中, 中药组治疗后有显著优势的Biomarker为Clostridium_sensu_stricto_1、Bacteroides_plebeius等; 西药组治疗后有显著优势的Biomarker为ruminococcus_gnavus_group。菌群功能预测提示, 理肠饮治疗IBS-D的主要途径为糖代谢相关途径。④治疗期间2组患者均未出现与药物相关的不良反应。 结论 中药复方理肠饮治疗IBS-D肝郁脾虚证疗效确切、安全, 其机制可能与调节血清脑肠肽水平、调整肠道菌群结构、纠正菌群失衡状态、调控糖代谢相关菌群有关。 Abstract:OBJECTIVE To observe the clinical efficacy of Lichang beverage in the treatment of diarrhea-type irritable bowel syndrome (IBS-D) based on the bacteria-brain-intestine axis and its effects on serum brain-gut peptide and intestinal flora, and to explore the possible mechanism of efficacy. METHODS A total of 66 IBS-D patients with liver depression and spleen deficiency were randomly divided into the Chinese medicine group (44 patients) and the western medicine group (22 patients) in a 2 ∶ 1 ratio. In the Chinese medicine group, Lichang beverage was given orally. However, the patients in the western medicine group were administrated with Bifico combination with Dicetel. The treatment course lasted four weeks. Besides, the changes in the IBS-SSS scores of both groups were evaluated before treatment, as well as after two weeks and four weeks of treatment. The changes in the traditional Chinese medicine (TCM) syndrome scores of both groups were observed before and after treatment. In addition, the expression levels of serum brain-gut peptide indexes [substance P (SP) and serotonin (5-HT)] and the composition of intestinal flora were measured. RESULTS The IBS-SSS scores of both groups were reduced significantly after two weeks and four weeks of treatment (P < 0.01), but the results in the Chinese medicine group were better than those in the western medicine group (P < 0.01). After four weeks of treatment, the total TCM syndrome scores of both groups were reduced significantly (P < 0.01), while the results in the Chinese medicine group were better than those in the western medicine group (P < 0.01). In addition, the clinical healing rate and total effective rate of the Chinese medicine group were higher than those of the western medicine group (P < 0.05, P < 0.01). After treatment, the serum SP level in both groups were reduced significantly (P < 0.05), and the serum 5-HT level in the Chinese medicine group were reduced notably (P < 0.01), but there was no significant difference between the two groups (P>0.05). The α diversity analysis indicated that the richness of intestinal flora in both groups decreased to different degrees after treatment (P < 0. 05, P < 0.01), and the diversity of flora in the western medicine group was reduced compared with that before (P < 0. 05), while there was no significant difference in the Chinese medicine group (P>0. 05). The PCoA analysis showed that the composition of microbial community in both groups changed significantly (P < 0. 05), and there were significant differences between groups (P < 0.01). Among them, the biomarkers with significant advantages after treatment in the Chinese medicine group were Clostridium_sensu_stricto_1 and Bacteroides_plebeius. However, the Biomarkers with significant advantages after treatment in the western medicine group were ruminococcus_gnavus_group. The functional prediction of the flora suggested that the main pathway of IBS-D treatment by Lichang beverage was glucose metabolism-related. Besides, no drug-related adverse reactions were observed in either group during the treatment course. CONCLUSION The efficacy of Chinese herbal medicine compound — Lichang beverage in treating IBS-D with liver depression and spleen deficiency is accurate and safe. Its mechanism may be related to the regulation of serum brain-gut peptide level, adjustment of intestinal flora structure, correction of flora imbalance, and regulation of glucose metabolism-related flora. -

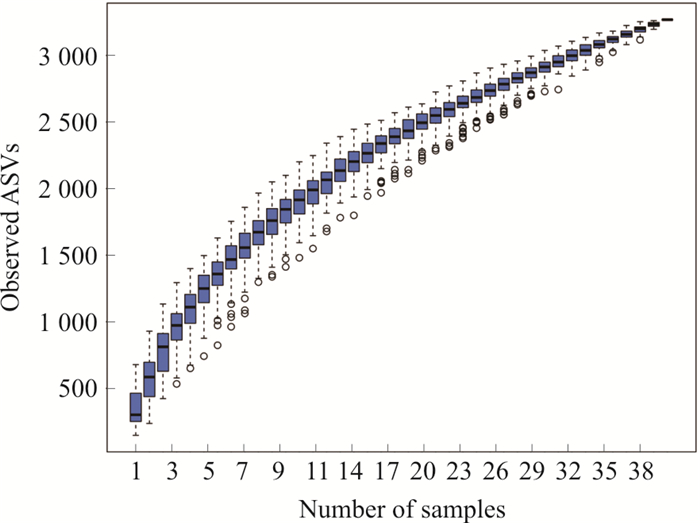
图 2 2组患者治疗前后肠道菌群多样性比较
注: BL.中药组治疗前; AL.中药组治疗后; BP.西药组治疗前; AP.西药组治疗后; 与本组治疗前相比, *P < 0.05, **P < 0.01。
Figure 2. Comparison of the diversity of intestinal flora in 2 groups before and after treatment
表 1 2组患者基线资料比较(x±s)
Table 1. Comparison of general data of the two groups of patients (x±s)
组别 例数 性别 年龄/岁 BMI/(kg·m-2) 婚姻状况 工作性质 学历 病程分布/月 男 女 已婚 未婚 体力 脑力 高中以下 专科以上 ≤24 24~60 ≥60 中药组 41 31 10 38.71±10.16 22.24±3.21 33 8 6 35 9 32 19 9 13 西药组 20 13 7 35.45±13.61 21.54±2.80 13 7 3 17 4 16 7 7 6  下载: 导出CSV
下载: 导出CSV
表 2 中医泄泻肝郁脾虚证积分评分标准
Table 2. Evaluation standard of TCM syndrome score
症状 0级 1级 2级 3级 腹胀腹痛 0分: 无症状 3分: 偶有轻微腹胀腹痛 6分: 腹胀腹痛较重,但能忍受 9分: 剧烈腹胀腹痛,不能忍受,需要药物控制 大便泄泻 0分: 无症状 3分: 大便不成形,每日3~4次 6分: 大便稀溏,每日5~10次 9分: 大便如水样,每日10次以上 腹痛欲泻泻后痛减 0分: 无症状 3分: 偶有发生 6分: 经常发作,遇精神刺激加重 9分: 每日发作 情志抑郁烦躁易怒 0分: 无症状 3分: 偶有情绪抑郁或急躁 6分: 易发情绪抑郁低落或烦躁易怒 9分: 经常情绪抑郁低落或烦躁易怒难以自控 胸胁胀痛 0分: 无症状 1分: 偶尔胀痛,0.5 h内可自行缓解 2分: 每天疼痛时间<2 h 3分: 呈持续痛,需服止痛药 嗳气 0分: 无症状 1分: 每日<4次 2分: 每日4~10次 3分: 每日>10次 食欲不振 0分: 无症状 1分: 食欲较差,食量较平时少1/3 2分: 食欲不佳,食量较平时少1/3以上 3分: 终日不欲进食,食量不到平时1/2 倦怠乏力 0分: 无症状 1分: 肢体稍倦,可坚持轻体力工作 2分: 四肢乏力,勉强坚持日常活动 3分: 全身无力,终日不愿活动
下载: 导出CSV
表 3 2组患者治疗前后IBS-SSS积分比较(x±s)
Table 3. Comparison of IBS-SSS scores between 2 groups before and after treatment (x±s)
组别 例数 治疗前 治疗2周 治疗4周 中药组 41 360.12±50.14 212.93±72.89**## 126.46±70.76**ΔΔ## 西药组 20 339.50±45.48 264.00±53.60** 208.00±79.68**ΔΔ 注: 组内比较,与治疗前比较,**P < 0.01,与治疗2周比较,ΔΔP < 0.01;组间比较, ##P < 0.01。
下载: 导出CSV
表 4 2组患者IBS-SSS积分临床疗效比较
Table 4. Comparison of clinical efficacy between 2 groups of patients
组别 例数 治愈 显效 有效 无效 愈显率/% 总有效率/% 中药组 41 8 17 14 2 60.98## 95.12%# 西药组 20 1 3 11 5 20.00 75.00% 注: 组间比较, χ愈显率2=9.050,##P < 0.01;χ总有效率2=5.358,#P < 0.05。
下载: 导出CSV
表 5 2组患者治疗前后中医证候积分情况比较[M(P25, P75)]
Table 5. Comparison of TCM syndrome scores between 2 groups before and after treatment [M(P25, P75)]
组别 时间 腹胀腹痛 大便泄泻 腹痛欲泻, 泻后痛减 情志抑郁, 烦躁易怒 中药组 治疗前 6.00(6.00, 7.50) 3.00(3.00, 6.00) 6.00(6.00, 9.00) 6.00(6.00, 6.00) (n=41) 治疗后 3.00(3.00, 3.00)** 0.00(0.00, 3.00)**## 3.00(3.00, 3.00)**## 3.00(3.00, 3.00)**## 西药组 治疗前 6.00(6.00, 6.00) 6.00(6.00, 6.00) 9.00(9.00, 9.00) 6.00(6.00, 8.25) (n=20) 治疗后 3.00(3.00, 3.00)** 3.00(3.00, 3.00)** 4.00(4.50, 6.00)** 3.00(3.00, 6.00)** 组别 时间 胸胁胀痛 嗳气 食欲不振 倦怠乏力 总积分 中药组 治疗前 1.00(1.00, 2.00) 2.00(2.00, 3.00) 1.00(1.00, 1.00) 1.00(1.00, 1.50) 29.90±5.15 (n=41) 治疗后 0.00(0.00, 1.00)** 1.00(1.00, 1.00)**## 0.00(0.00, 0.00)**## 0.00(0.00, 1.00)**# 9.20±4.95**## 西药组 治疗前 1.00(1.00, 1.00) 2.00(2.00, 2.00) 1.00(1.00, 1.00) 1.00(1.00, 1.00) 30.20±5.22 (n=20) 治疗后 0.00(0.00, 1.00)* 2.00(2.00, 2.00) 1.00(1.00, 1.00) 1.00(1.00, 1.00)* 18.05±6.68**## 注: 组内比较, *P < 0.05, **P < 0.01;组间比较, #P < 0.05, ##P < 0.01。
下载: 导出CSV
表 6 2组患者治疗前后血清SP、5-HT含量比较(x±s, n=10)
Table 6. Comparison of serum SP and 5-HT levels in 2 groups before and after treatment (x±s, n=10)
组别 时间 SP/(pg·mL-1) 5-HT/(ng·mL-1) 中药组 治疗前 22.75±2.77 135.79±12.48 治疗后 19.07±2.47* 105.64±12.66** 西药组 治疗前 22.48±2.71 125.76±13.44 治疗后 18.25±2.36* 106.99±18.38 注: 组内比较, *P < 0.05, **P < 0.01。
下载: 导出CSV
-
[1] ENCK P, AZIZ Q, BARBARA G, et al. Irritable bowel syndrome[J]. Nat Rev Dis Primers, 2016, 2: 16014. doi: 10.1038/nrdp.2016.14 [2] XIONG LS, CHEN MH, CHEN HX, et al. A population-based epidemiologic study of irritable bowel syndrome in Guangdong province[J]. Nat Med J Chin, 2004, 84(4): 278-281. [3] 方秀才. 肠易激综合征发病机制研究进展[J]. 胃肠病学, 2020, 25(6): 321-325. doi: 10.3969/j.issn.1008-7125.2020.06.001FANG XC. Advances in study on pathogenesis of irritable bowel syndrome[J]. Chin J Gastroenterol, 2020, 25(6): 321-325. doi: 10.3969/j.issn.1008-7125.2020.06.001 [4] MARGOLIS KG, CRYAN JF, MAYER EA. The microbiota-gut-brain axis: From motility to mood[J]. Gastroenterology, 2021, 160(5): 1486-1501. doi: 10.1053/j.gastro.2020.10.066 [5] BENNETT G, TALLEY NJ. Irritable bowel syndrome in the elderly[J]. Best Pract Res Clin Gastroenterol, 2002, 16(1): 63-76. doi: 10.1053/bega.2001.0266 [6] 熊理守, 彭穗, 陈为, 等. 肠易激综合征患者的就医行为及其影响因素[J]. 中华全科医师杂志, 2010, 9(12): 829-832. doi: 10.3760/cma.j.issn.1671-7368.2010.12.006XIONG LS, PENG S, CHEN W, et al. Correlates of health-care seeking behavior in patients with irritable bowel syndrome[J]. Chin J Gen Pract, 2010, 9(12): 829-832. doi: 10.3760/cma.j.issn.1671-7368.2010.12.006 [7] 杨焱麟, 陈敏, 周彦妮, 等. P物质与肝郁脾虚型腹泻型肠易激综合征关系及中医药调控的研究进展[J]. 中华中医药学刊, 2021, 39(9): 82-85. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYHS202109022.htmYANG YL, CHEN M, ZHOU YN, et al. Research progress of substance P, liver stagnation and spleen deficiency type of IBS-D and traditional Chinese medicine regulation[J]. Chin Arch Tradit Chin Med, 2021, 39(9): 82-85. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYHS202109022.htm [8] 陈立亚, 刘畅, 汪芳裕. 肠易激综合征与肠道微生态及脑-肠轴关系的研究进展[J]. 胃肠病学和肝病学杂志, 2017, 26(5): 491-495. doi: 10.3969/j.issn.1006-5709.2017.05.004CHEN LY, LIU C, WANG FY. Research progress of the relationship of gut microbiota, gut-brain axis with irritable bowel syndrome[J]. Chin J Gastroenterol Hepatol, 2017, 26(5): 491-495. doi: 10.3969/j.issn.1006-5709.2017.05.004 [9] TAP J, DERRIEN M, TÖRNBLOM H, et al. Identification of an intestinal microbiota signature associated with severity of irritable bowel syndrome[J]. Gastroenterology, 2017, 152(1): 111-123. doi: 10.1053/j.gastro.2016.09.049 [10] LABUS JS, OSADCHIY V, HSIAO EY, et al. Evidence for an association of gut microbial Clostridia with brain functional connectivity and gastrointestinal sensorimotor function in patients with irritable bowel syndrome, based on tripartite network analysis[J]. Microbiome, 2019, 7: 45. doi: 10.1186/s40168-019-0656-z [11] BARBARA G, FEINLE-BISSET C, GHOSHAL UC, et al. The intestinal microenvironment and functional gastrointestinal disorders[J]. Gastroenterology, 2016, 150(6): 1305-1318. doi: 10.1053/j.gastro.2016.02.028 [12] 李兆龙, 张有成, 韩文峰, 等. 粪菌移植治疗肠易激综合征研究进展[J]. 中国微生态学杂志, 2021, 33(2): 231-235. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWS202102023.htmLI ZL, ZHANG YC, HAN WF, et al. Advances in the treatment of irritable bowel syndrome with fecal bacteria transplantation[J]. Chin J Microecol, 2021, 33(2): 231-235. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWS202102023.htm [13] 赵鲁卿, 张声生, 卢小芳, 等. 疏肝健脾方对腹泻型肠易激综合征大鼠的治疗作用及对肥大细胞、5-HT通路的影响[J]. 中国中西医结合消化杂志, 2017, 25(8): 589-594. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXPW201708009.htmZHAO LQ, ZHANG SS, LU XF, et al. Effect of Shugan Jianpi formula on mast cell and 5-HT pathway in D-IBS rats[J]. Chin J Integr Tradit West Med Dig, 2017, 25(8): 589-594. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXPW201708009.htm [14] 孙大娟, 由新鹏, 迟莉丽. 基于"土中泻木"理论论治肝郁脾虚型腹泻型肠易激综合征疗效观察及机制探讨[J]. 南京中医药大学学报, 2020, 36(2): 193-196. http://xb.njucm.edu.cn/article/id/zr20200213SUN DJ, YOU XP, CHI LL. Discussion on curative effect and mechanism of treating diarrhea predominant irritable bowel syndrome with liver-stagnation and spleen-deficiency based on"purging wood from earth"[J]. J Nanjing Univ Tradit Chin Med, 2020, 36(2): 193-196. http://xb.njucm.edu.cn/article/id/zr20200213 [15] 孙大娟, 梁峻尉, 闫华, 等. 腹泻型肠易激综合征患者直肠动力学变化及中药复方的干预作用[J]. 中国中医药科技, 2019, 26(3): 423-424. https://www.cnki.com.cn/Article/CJFDTOTAL-TJYY201903044.htmSUN DJ, LIANG JW, YAN H, et al. Rectal dynamic change in patients with diarrhea-predominant irritable bowel syndrome and that intervention effect of chinese herbal compound[J]. Chin J Tradit Med Sci Technol, 2019, 26(3): 423-424. https://www.cnki.com.cn/Article/CJFDTOTAL-TJYY201903044.htm [16] 孙大娟, 迟莉丽, 梁峻尉, 等. 焦虑状态与IBS-D的相关性研究及中药复方的干预作用[J]. 光明中医, 2018, 33(17): 2473-2475. doi: 10.3969/j.issn.1003-8914.2018.17.004SUN DJ, CHI LL, LIANG JW, et al. Study on the correlation between anxiety state and IBS-D and intervention effect of compound traditional Chinese medicine[J]. Guangming J Chin Med, 2018, 33(17): 2473-2475. doi: 10.3969/j.issn.1003-8914.2018.17.004 [17] 梁峻尉, 白文筠, 迟莉丽, 等. 加味理肠饮对腹泻型肠易激综合征大鼠5-HT、NPY及肥大细胞的影响[J]. 山东中医药大学学报, 2018, 42(4): 346-350. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYX201804023.htmLIANG JW, BAI WJ, CHI LL, et al. Effects of Jiawei lichang decoction on 5-HT, NPY, and mast cells in rats with diarrhea-predominant irritable bowel syndrome[J]. J Shandong Univ Tradit Chin Med, 2018, 42(4): 346-350. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYX201804023.htm [18] 梁峻尉, 白文筠, 迟莉丽, 等. 中药加味理肠饮对腹泻型肠易激综合征大鼠SP、VIP、CORT含量的影响[J]. 中医药学报, 2018, 46(3): 54-57. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXB201803014.htmLIANG JW, BAI WY, CHI LL, et al. Effect of modified Jiawei lichang Yin on SP, VIP and CORT in IBS rats of diarrhea type[J]. Acta Chin Med Pharmacol, 2018, 46(3): 54-57. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXB201803014.htm [19] 王雨宁, 徐畅, 邹康, 等. 临床试验中适应性随机化的应用[J]. 中国循证医学杂志, 2020, 20(5): 616-620. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZXZ202005017.htmWANG YN, XU C, ZOU K, et al. Application of adaptive randomization in clinical trials[J]. Chin J Evid Based Med, 2020, 20(5): 616-620. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZXZ202005017.htm [20] DROSSMAN DA, HASLER WL. Rome Ⅳ—functional GI disorders: Disorders of gut-brain interaction[J]. Gastroenterology, 2016, 150(6): 1257-1261. doi: 10.1053/j.gastro.2016.03.035 [21] 中药新药临床研究指导原则(试行)[M]. 北京: 中国医药科技出版社, 2002: 134-151.Guiding Principles for Clinical Research of New Chinese Medicine: Trial Implementation[M]. Beijing: China medical science press, 2002: 134-151. [22] 张声生, 魏玮, 杨俭勤. 肠易激综合征中医诊疗专家共识意见(2017)[J]. 中医杂志, 2017, 58(18): 1614-1620. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZYZ201718024.htmZHANG SS, WEI W, YANG JQ. Consensus of TCM diagnosis and treatment experts on irritable bowel syndrome(2017)[J]. J Tradit Chin Med, 2017, 58(18): 1614-1620. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZYZ201718024.htm [23] 卞立群. 肠安Ⅰ号方治疗IBS-D的临床疗效评价暨临床疗效评价指标的比较研究[D]. 北京: 中国中医科学院, 2011.BIAN LQ. Clinical effect evaluation of Chang'anyihao decoction in treating IBS-D and research of IBS clinical effect assessment indices[D]. Beijing: China Academy of Chinese Medical Sciences, 2011. [24] GROS M, GROS B, MESONERO JE, et al. Neurotransmitter dysfunction in irritable bowel syndrome: Emerging approaches for management[J]. J Clin Med, 2021, 10(15): 3429. doi: 10.3390/jcm10153429 [25] MISHIMA Y, ISHIHARA S. Enteric microbiota-mediated serotonergic signaling in pathogenesis of irritable bowel syndrome[J]. Int J Mol Sci, 2021, 22(19): 10235. doi: 10.3390/ijms221910235 [26] 胡莹, 郑依玲, 梅全喜, 等. 痛泻要方破壁饮片对腹泻型肠易激综合征大鼠脑肠肽的影响[J]. 中药材, 2020, 43(7): 1726-1731. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYCA202007036.htmHU Y, ZHENG YL, MEI QX, et al. Effect of Tongxieyaofang ultrafine granular powder on intestine propulsion and vasoactive intestinal peptide in diarrhea-predominant of irritable bowel syndrome model rats[J]. J Chin Med Mater, 2020, 43(7): 1726-1731. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYCA202007036.htm [27] BOSI A, BANFI D, BISTOLETTI M, et al. Tryptophan metabolites along the microbiota-gut-brain axis: An interkingdom communication system influencing the gut in health and disease[J]. Int J Tryptophan Res, 2020, 13: 1178646920928984. [28] KONG C, GAO RY, YAN XB, et al. Probiotics improve gut microbiota dysbiosis in obese mice fed a high-fat or high-sucrose diet[J]. Nutrition, 2019, 60: 175-184. doi: 10.1016/j.nut.2018.10.002 [29] PÉREZ-BURILLO S, PASTORIZA S, FERNáNDEZ-ARTEAGA A, et al. Spent coffee grounds extract, rich in mannooligosaccharides, promotes a healthier gut microbial community in a dose-dependent manner[J]. J Agric Food Chem, 2019, 67(9): 2500-2509. doi: 10.1021/acs.jafc.8b06604 [30] XIAO L, LIU Q, LUO M, et al. Gut microbiota-derived metabolites in irritable bowel syndrome[J]. Front Cell Infect Microbiol, 2021, 11: 729346. doi: 10.3389/fcimb.2021.729346 [31] HALMOS EP, POWER VA, SHEPHERD SJ, et al. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome[J]. Gastroenterology, 2014, 146(1): 67-75. doi: 10.1053/j.gastro.2013.09.046 [32] CREMON C, CARINI G, WANG BX, et al. Intestinal serotonin release, sensory neuron activation, and abdominal pain in irritable bowel syndrome[J]. Am J Gastroenterol, 2011, 106(7): 1290-1298. doi: 10.1038/ajg.2011.86 [33] 唐洪梅, 涂星, 柴玉娜, 等. 两种亚型肠易激综合征中氨基酸神经递质及其受体变化[J]. 世界华人消化杂志, 2014, 22(30): 4559-4565. https://www.cnki.com.cn/Article/CJFDTOTAL-XXHB201430002.htmTANG HM, TU X, CHAI YN, et al. Contents of amino acid neurotransmitters and expression of γ-aminobutyric acid receptor in two subtypes of irritable bowel syndrome[J]. World Chin J Dig, 2014, 22(30): 4559-4565. https://www.cnki.com.cn/Article/CJFDTOTAL-XXHB201430002.htm [34] 赵滢. 抗生素诱导小鼠菌群变化与宿主代谢组相关性的研究[D]. 武汉: 华中科技大学, 2013.ZHAO Y. Antibiotics-induced mice microbial alteration and their relationship with host metabolic profiles[D]. Wuhan: Huazhong University of Science and Technology, 2013. [35] CHAVES FILHO AJM, LIMA CNC, VASCONCELOS SMM, et al. IDO chronic immune activation and tryptophan metabolic pathway: A potential pathophysiological link between depression and obesity[J]. Prog Neuro Psychopharmacol Biol Psychiatry, 2018, 80: 234-249. doi: 10.1016/j.pnpbp.2017.04.035 [36] HATA T, ASANO Y, YOSHIHARA K, et al. Regulation of gut luminal serotonin by commensal microbiota in mice[J]. PLoS One, 2017, 12(7): e0180745. doi: 10.1371/journal.pone.0180745 [37] ALEMI F, POOLE DP, CHIU J, et al. The receptor TGR5 mediates the prokinetic actions of intestinal bile acids and is required for normal defecation in mice[J]. Gastroenterology, 2013, 144(1): 145-154. doi: 10.1053/j.gastro.2012.09.055 [38] REIGSTAD CS, SALMONSON CE, RAINEY JF, et al. Gut microbes promote colonic serotonin production through an effect of short-chain fatty acids on enterochromaffin cells[J]. FASEB J, 2015, 29(4): 1395-1403. doi: 10.1096/fj.14-259598 -



 点击查看大图
点击查看大图
计量
- 文章访问数: 202
- HTML全文浏览量: 49
- PDF下载量: 30
- 被引次数: 0
