

Exploring the Correlation between Syndrome Differentiation of Traditional Chinese Medicine of Non-Ischemic Cardiomyopathy and Myocardial Fibrosis Based on Cardiac MRI
-
摘要: 目的 探讨非缺血性心肌病(NICM)中医不同辨证分型与心脏容积、功能参数及心肌纤维化的相关性。方法 选择2019年9月至2020年10月南方医科大学顺德医院临床确诊为NICM患者64例。按中医辨证分型分为3组, 包括心血瘀阻证组、痰浊痹阻证组、非心血瘀阻非痰浊痹阻证组(包括心阳不振证、心肾阴虚证、气阴两虚证、寒凝心脉证)。所有患者行心脏磁共振检查(CMR), 扫描包括黑血序列、亮血序列及延迟增强扫描(LGE)。CMR亮血序列图像经后处理获得心脏容积和功能等参数, 包括左心室射血分数(LVEF)、左心室舒张末期容积指数(LVEDVI)、左心室收缩末期容积指数(LVESVI)、左心室每搏量(LVSVI)、左心室心排出量(LVCOI)及左心室质量指数(LVMMI)。LGE左心室图像按美国心脏协会(AHA)推荐分为17节段, 并根据心室壁异常强化的节段分布, 分为1~3级。对以上数据进行统计学分析。结果 痰浊痹阻证组与非心血瘀阻非痰浊痹阻证组LVEF比较, 差异有统计学意义(P < 0.05);痰浊痹阻证组与心血瘀阻证组、非心血瘀阻非痰浊痹阻证组LVEDVI比较, 差异有统计学意义(P < 0.05, P < 0.01);痰浊痹阻证组与非心血瘀阻非痰浊痹阻证组LVESVI比较, 差异有统计学意义(P < 0.01)。心血瘀阻证组与痰浊痹阻证组心肌纤维化程度比较, 差异有统计学意义(P < 0.05)。结论 NICM不同辨证分型与心脏容积、功能参数及心肌纤维化程度有一定相关性, 通过运用现代磁共振技术对中医辨证分型进行半定量化、定量化研究, 为其客观化研究提供了新思路, 为揭示中医学的本质提供了新方法。Abstract: OBJECTIVE To investigate the correlation between syndrome differentiation of traditional Chinese medicine (TCM) of non-ischemic cardiomyopathy (NICM) and parameters of the cardiac volume and function, along with myocardial fibrosis.METHODS We selected 64 patients clinically diagnosed with NICM from September 2019 to October 2020 at Shunde Hospital of Southern Medical University. The patients were divided into three groups according to TCM syndrome differentiation, including the syndrome of stasis obstructing the heat blood, syndrome of turbid phlegm obstruction, as well as the syndrome of neither stasis obstructing the heat blood nor turbid phlegm obstruction (heart yang insufficiency, heart-kidney yin deficiency, deficiency of both qi and yin, and cold congealing heart vessel). All patients underwent cardiac magnetic resonance (CMR), which includes black-blood sequence, bright-blood sequence, and late gadolinium enhancement (LGE). The CMR bright-blood sequence images were post-processed to obtain parameters of cardiac volume and function, including left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume index (LVEDVI), left ventricular end-systolic volume index (LVESVI), left ventricular stroke volume index (LVSVI), left ventricular cardiac output index (LVCOI), and left ventricular mass index (LVMI). The LGE left ventricular images were divided into 17 segments according to the American Heart Association (AHA) recommendations and were classified into grades one to three according to the segmental distribution of abnormal ventricular wall enhancement. In addition, statistical analysis was performed on the above data.RESULTS The differences were statistically significant (P < 0.05) when comparing the LVEF in the turbid phlegm obstruction group and neither stasis obstructing the heat blood nor turbid phlegm obstruction groups. The differences were statistically significant (P < 0.05, P < 0.01) when comparing the LVEDVI in the turbid phlegm obstruction group, the stasis obstructing the heat blood group, as well as neither stasis obstructing the heat blood nor turbid phlegm obstruction groups. The differences were statistically significant (P < 0.01) when comparing the LVESVI in the turbid phlegm obstruction group and neither stasis obstructing the heat blood nor turbid phlegm obstruction groups. The difference was statistically significant (P < 0.05) when comparing myocardial fibrosis degree in the stasis obstructing the heat blood group with the turbid phlegm obstruction group.CONCLUSION The TCM syndrome differentiation of NICM has some correlation with parameters of the cardiac volume and function as well as myocardial fibrosis degree. Thus, this study provides new ideas for objective research and new methods for revealing the essence of Chinese medicine through the semi-quantitative and quantitative study of TCM syndrome differentiation combined with modern magnetic resonance technology.
-

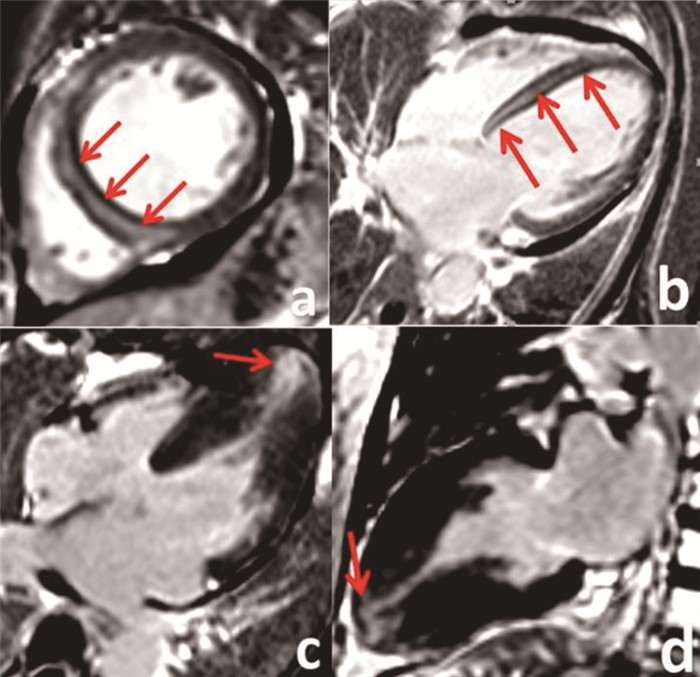
图 1 NICM患者的CMR图像
注: a~b.患者男, 67岁, 扩张型心肌病, 心血瘀阻证组, 磁共振延迟增强显示室间隔广泛心肌纤维疤痕形成(红色箭头); c~d.患者男, 67岁, 肥厚型心肌病, 痰浊痹阻证组, 磁共振延迟增强显示心尖部少量心肌纤维疤痕形成(红色箭头)。
表 1 3组心功能参数的比较x±s
组别 例数 LVEF/% LVEDVI/mL LVESVI/mL LVSVI/(mL·m-2) LVCOI/(L·min-1) LVMMI/(g·m-2) 心血瘀阻证组 17 44.8±19.9 208.5±98.6# 176.4±113.2 75.7±17.4 5.3±1.1 168.8±67.2 痰浊痹阻证组 27 38.7±17.4 261.8±85.8 202.9±73.0 89.3±26.6 6.2±2.3 194.0±55.0 非心血瘀阻非痰浊痹阻证组 20 50.5±15.9# 160.3±54.9## 99.4±54.7## 79.7±29.6 5.1±1.6 164.8±64.4 注: 与痰浊痹阻证组比较, #P < 0.05, ##P < 0.01。  下载: 导出CSV
下载: 导出CSV
表 2 3组心肌纤维化的比较x±s
组别 例数 左室心肌纤维化分级 左室心肌纤维化率/% 1级 2级 3级 心血瘀阻证组 17 4 2 11 76.47# 痰浊痹阻证组 27 14 8 5 48.15 非心血瘀阻非痰浊痹阻证组 20 8 6 6 60.00 注: 心血瘀阻证组与痰浊痹阻证组经Kruskal-Wallis检验比较, 采用Bonferroni法校正, H=14.723, #P < 0.05。
下载: 导出CSV
-
[1] MAURICIO P, EDUARDO RL, ANDRE Z, et al. Sudden cardiac death markers in non-ischemic cardiomyopathy[J]. J Electrocardiol, 2016, 49(3): 446-451. doi: 10.1016/j.jelectrocard.2016.03.012 [2] 国家技术监督局. 中医临床诊疗术语(疾病部分): GB/T 16751.1-1997[S/OL]. [2021-08-29]. https://max.book118.com/html/2019/0418/8025106105002017.shtm. [3] 罗文杰, 吴焕林, 王侠, 等. 冠心病证候诊断方法及分型文献研究[J]. 中国中西医结合杂志, 2012, 32(6): 843-845. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZXJ201206041.htm [4] 于海峰. 从心痹辨治扩张型心肌病的体会[J]. 上海中医药杂志, 2014, 48(1): 61-62. https://www.cnki.com.cn/Article/CJFDTOTAL-SHZZ201401029.htm [5] SEGURA AM, FRAZIER OH, BUJA LM. Fibrosis and heart failure[J]. Heart Fail Rev, 2014, 19(2): 173-185. doi: 10.1007/s10741-012-9365-4 [6] 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会, 中国心肌病诊断与治疗建议工作组. 心肌病诊断与治疗建议[J]. 中华心血管病杂志, 2007, 35(1): 5-16. doi: 10.3760/j:issn:0253-3758.2007.01.003 [7] 周仲瑛. 中医内科学[M]. 北京: 中国中医药出版社, 2012: 407-409. [8] 胸痹心痛的诊断依据、证候分类、疗效评定: 中华人民共和国中医药行业标准《中医内科病证诊断疗效标准》(ZY/T001.1-94)[J]. 辽宁中医药大学学报, 2016, 18(7): 32. https://www.cnki.com.cn/Article/CJFDTOTAL-LZXB201607011.htm [9] ELOISA A, NAVNEET N, WILLIAM DG, et al. The MOGE(S)classification for a phenotype-genotype nomenclature of cardiomyopathy: endorsed by the World Heart Federation[J]. J Am Coll Cardiol, 2013, 62(22): 2046-2072. doi: 10.1016/j.jacc.2013.08.1644 [10] 刘文华, 唐少华, 许静芳, 等. 经典理论指导辨证治疗胸痹的临床体会[J]. 辽宁中医杂志, 2011, 38(2): 264-266. https://www.cnki.com.cn/Article/CJFDTOTAL-LNZY201102030.htm [11] ILES L, PFLUGER H, LEFKOVITS L, et al. Myocardial fibrosis predicts appropriate device therapy in patients with implantable cardioverter-defibrillators for primary prevention of sudden cardiac death[J]. J Am Coll Cardiol, 2011, 57(7): 821-828. doi: 10.1016/j.jacc.2010.06.062 [12] 丁然, 陆小左. 基于有无痛胸分型的胸痹脉象中医客观化研究[J]. 中医药信息, 2018, 35(2): 66-69. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXN201802017.htm [13] 唐宗海. 血证论[M]. 天津: 天津科学技术出版社, 2003: 85. [14] 韦红, 阎国良, 李越华. 从痰瘀论治心肌纤维化的机理初探[J]. 陕西中医药大学学报, 2019, 42(1): 38-39, 46. https://www.cnki.com.cn/Article/CJFDTOTAL-SXXY201901014.htm -

 点击查看大图
点击查看大图
图(1) / 表(2)
计量
- 文章访问数: 189
- HTML全文浏览量: 30
- PDF下载量: 97
- 被引次数: 0
